.png)
Treatment Options
Surgery
The main treatment for endometrial cancer is surgery to remove the womb and cervix (called a ‘total hysterectomy’), fallopian tubes and ovaries (called ‘salpingo-oophorectomy’). Your surgeon may also remove lymph nodes and a layer of fat at the front of abdomen (called the ‘omentum’) and check organs nearby to find if the cancer has spread.
A hysterectomy can be done in different ways. The main two options are:
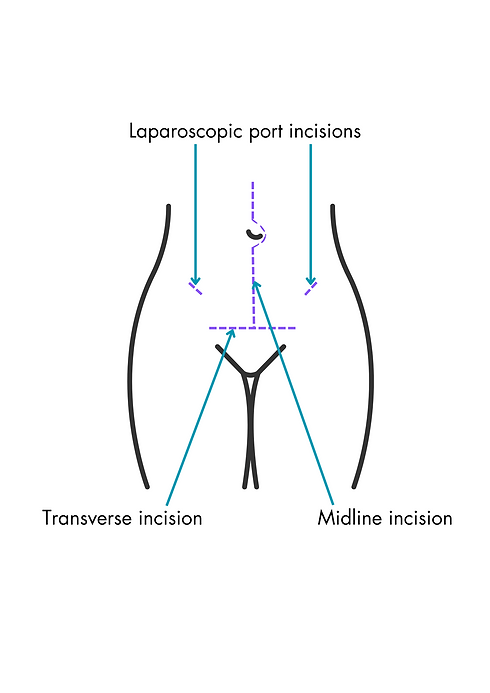
- keyhole (laparoscopic), where small cuts in the tummy are made for a small video camera and surgical instruments to be used, and
- open (abdominal), where the surgeon makes one cut in the tummy, usually close to the bikini line.
See opposite for how different incisions (cuts) are made on the tummy.
Vaginal hysterectomies are not usually conducted in the case of endometrial cancer as the Fallopian tubes and ovaries are removed in addition to the uterus and cervix.
As performed in the case of biopsies, your womb, cervix, fallopian tubes and ovaries removed at surgery will be examined by a pathologist under the microscope. He/she will diagnose the type of cancer present and provide both a definitive stage (a measure of how far the cancer has spread) and a grade (a measure of how aggressive the cancers cells look). In turn, this will determine the subsequent course of treatment.
It is important to note that the surgery and postoperative treatment is determined by a panel of clinical experts from different subspecialities, including surgeons, radiologists, pathologists, and medical and clinical oncologists and is not decided by any one doctor in isolation.
If you are still having regular periods, removing your ovaries will lead to symptoms of the menopause after your surgery which may be much earlier than normal for you. Your doctor will discuss different treatment options with you.
Other Treatments
After surgery, your doctor may advise other treatments to reduce the risk of cancer returning (adjuvant treatment).
In a minority of cases, if your CT or MRI scans show that the cancer has spread extensively (Stage 4), you may be offered primary chemotherapy before surgery (this is called ‘neoadjuvant therapy’).
Specific Situations
.png)
Fertility-sparing treatment
This is only suitable for women with Stage 1, Grade 1 endometrial cancer in a few specialist centres. It usually involves either taking daily progesterone tablets and/or inserting a progesterone releasing coil into the womb. You will have regular checks (more endometrial biopsies over the course of time) and your doctor will discuss the risks and benefits with you prior to agreeing to this treatment. This allows you to retain your fertility. In these cases, after you have children or if the cancer does not respond to the treatment, you will still be advised to have a hysterectomy.

Advanced cancer
For patients who have cancer that has spread to other parts of the body, chemotherapy or hormonal therapy is used (in this context, surgery is only ever rarely used). The aim of this treatment is to help relieve your symptoms and shrink the cancer. This is known as palliative treatment. People may feel better and live longer but unfortunately this treatment will not cure the cancer.